The CMS 900-minute rule — formally codified as the "intensive rehabilitation therapy" requirement in the Medicare Benefit Policy Manual, Chapter 1, Section 110 — sets the threshold below which an Inpatient Rehabilitation Facility stay can be denied as not "reasonable and necessary" under Medicare Part A [1][2]. CMS data from 2024 shows medical necessity accounted for 93.8% of improper payments in inpatient rehabilitation hospitals during that reporting period, with documentation deficiencies driving most of the rest [3]. We work with rehab hospital leaders across the country, and the IRFs achieving 95% reimbursement approval share the same operational backbone — automated, real-time scheduling that adapts to refusals, cancellations, and make-up minutes without nightly manual rebuilds [Opmed]. Below, we explain the 900-minute rule in plain regulatory language, the audit risks of getting it wrong in 2026, and the operational changes that move IRFs from manual schedule rebuilds to continuous compliance.
🎯 Key Takeaways
- The rule is 3 hours per day, 5 days per week — or 15 hours over 7 days: CMS Medicare Benefit Policy Manual §110 specifies that intensive rehabilitation therapy "consists of at least 3 hours of therapy per day at least 5 days per week," with an alternative path of "at least 15 hours of therapy per week" (900 minutes) for patients whose clinical condition requires a different distribution [1]
- Therapy must begin within 36 hours of admission: Per 42 CFR § 412.622(a)(3)(ii), the required therapy treatments must begin within 36 hours from midnight of the day of admission to the IRF [4]
- Audit pressure is intensifying in 2026: CMS expanded its IRF Review Choice Demonstration to Texas (March 2, 2026) and California (May 1, 2026), requiring participating IRFs to choose between 100% pre-claim review or 100% postpayment review [5]
- The financial stakes are real: the average IRF FY2026 PPS per-discharge payment is approximately $19,364, and IRFs that fail QRP reporting face a 2-percentage-point reduction in their Annual Increase Factor [6][7]
- CMS error rates were historically high: the Comprehensive Error Rate Testing (CERT) program found IRF error rates rose from 9% in 2012 to 62% in 2016, prompting the still-ongoing OIG nationwide IRF audit announced in 2022 [8][9]
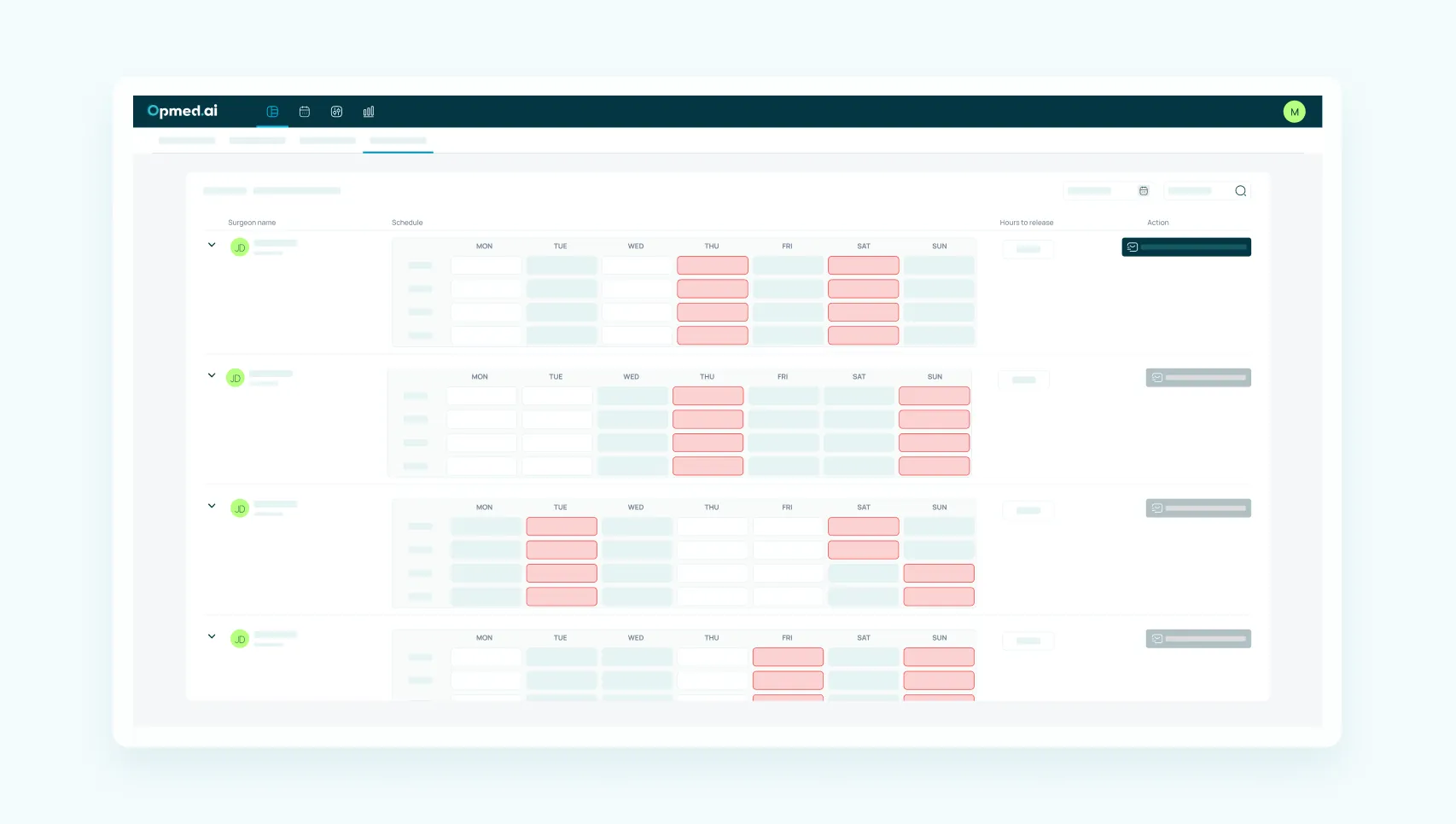
- Compliance is an operations problem: the rule fails at execution, not at clinical capability — intraday schedule drift, refusals, and make-up minute coordination compound faster than nightly manual schedule rebuilds can absorb [Opmed IRF Handout 2026]
What the CMS 900-Minute Rule Actually Says
The "900-minute rule" is industry shorthand for the intensive rehabilitation therapy requirement set out in Section 110 of the Medicare Benefit Policy Manual and codified in 42 CFR § 412.622. The 900-minute number itself comes from the alternative path: 15 hours × 60 minutes = 900 minutes over a 7-consecutive-calendar-day period [1].
CMS frames the requirement two ways:
"Although the intensity of rehabilitation services can be reflected in various ways, the generally-accepted standard by which the intensity of these services is typically demonstrated in IRFs is by the provision of intensive therapies at least 3 hours per day at least 5 days per week."
— Medicare Benefit Policy Manual, Chapter 1, Section 110, Centers for Medicare & Medicaid Services [1]
The first path (3 hours × 5 days) and the alternative path (15 hours over 7 days) both equal the same 900 minutes — the difference is distribution. The alternative path exists because some patients can't tolerate 3 hours of therapy on a daily schedule due to medical complexity, treatment side effects, or recovery patterns. CMS allows the 7-day window to give clinical teams flexibility while preserving the therapy intensity threshold.
The therapy must be delivered across multiple disciplines — physical therapy, occupational therapy, speech-language pathology, or prosthetics and orthotics — with at least one being PT or OT. Group therapy is permitted as an adjunct to one-on-one therapy, but the standard of care under CMS guidance remains individualized therapy [1].
What "Reasonable and Necessary" Means in IRF Audits
The 900-minute rule is one component of a broader "reasonable and necessary" determination CMS makes when reviewing IRF claims. The other elements:
- Pre-admission screening documenting the patient's expected need for intensive rehabilitation [1]
- Physician’s History and Physical (H&P) , completed and signed within 24 hours of admission [1]
- Individualized overall plan of care specifying expected intensity, frequency, and duration of interventions, signed by a rehabilitation physician [1]
- Interdisciplinary team conferences at least weekly, led by a rehabilitation physician [1]
- Face-to-face physician visits at least 3 days per week throughout the stay (after the first week, a non-physician practitioner may conduct one of the three) [1]
When CMS, the OIG, or a Medicare Administrative Contractor reviews an IRF claim, the 900-minute threshold is one of several documentation elements they verify. Failing any single element can put the entire stay's reimbursement at risk [10].
Why 900-Minute Compliance Is Harder Than It Looks
In an idealized week, every patient receives uninterrupted 3-hour therapy blocks across 5 days, every therapist is available, and no one refuses, falls ill, or leaves early. In real IRFs, none of those things hold true.
The pattern we see across rehab hospital leaders: 4–5 hours per day of manual scheduling work spread across multiple staff members, coordinating refusals, cancellations, make-up minutes, and therapist availability — only to start over the next morning [Opmed IRF Handout 2026]. 85% of therapists say scheduling overhead delays patient progress, driving discharge delays, missed family training, and lower satisfaction scores [Opmed IRF Handout 2026]. The compounding effect on staff is measurable: rehab therapy turnover runs at approximately 12% annually, with 49% of therapists reporting significant burnout, and replacing a single IRF therapist costs an estimated $30,000–$50,000 [Opmed IRF Handout 2026].
The math is unforgiving. A 50-bed IRF running near capacity sees roughly 200 Medicare patients across a quarter. Each patient generates a rolling 7-day window of compliance obligations. With an average length of stay near 12–13 days, every patient has at least one full 7-day compliance window plus a partial second window. That's 200+ separate compliance evaluations per quarter — and they're all running simultaneously, with different start dates, different therapy mixes, and different clinical complexity profiles.
Where Compliance Actually Breaks Down
Across our customer base, four operational failure points account for the majority of 900-minute misses:
- Late therapy initiation. CMS requires therapy to start within 36 hours of midnight on the day of admission [4]. When admission paperwork, evaluations, or initial documentation slip past that window, the patient enters Day 2 already short on minutes — and the entire 7-day calculation starts behind.
- Refusal and cancellation cascades. When a patient refuses a session or a therapist calls out, manual schedules typically can't reabsorb the impact in real time. Make-up minutes get pushed to "later in the week," and "later" becomes "Saturday" when the schedule has the least flexibility.
- Cross-discipline coordination gaps. PT, OT, and SLP availability rarely align cleanly. A 3-hour day requires sequencing across all three disciplines without overlap, with appropriate rest intervals, in a finite number of treatment rooms. Manual schedulers solve this for tomorrow, then rebuild from scratch when reality diverges.
- End-of-week recovery exercises. When schedule drift accumulates through Wednesday and Thursday, IRFs run "compliance recovery" sessions on Friday and Saturday — but those sessions are exactly when therapist availability is lowest and patient fatigue is highest.
Each of these 4 failure points is an operational problem, not a clinical one. The clinical teams know what therapy patients need; the breakdown is in matching capacity to obligation in real time.
The 2026 Audit Landscape: Why Compliance Pressure Is Intensifying
CMS and OIG audit activity around IRFs has accelerated meaningfully in the last 24 months. Three developments matter for IRF leaders planning compliance posture in 2026:
The Review Choice Demonstration is expanding. CMS launched the IRF Review Choice Demonstration (RCD) in Alabama (August 2023) and Pennsylvania (June 2024), requiring IRFs in those states to choose between 100% pre-claim review or 100% postpayment review of Medicare claims [5]. CMS announced expansion to Texas effective March 2, 2026 and California effective May 1, 2026 — bringing four high-volume IRF states under structured review [5]. After 6 months of demonstrated compliance, IRFs become eligible for additional review choices with reduced burden, but the entry point requires every claim to be reviewable on documentation alone.
The OIG's nationwide audit is ongoing. In 2022, OIG announced a follow-up to its 2018 nationwide IRF audit, which had found that medical record documentation for 175 of 220 sampled IRF stays did not support that the care was "reasonable and necessary" under Medicare requirements [10]. That 2018 finding was contested by the American Hospital Association on methodological grounds — particularly around the OIG's extrapolation from 220 audited claims to a $5.7 billion estimated improper payment figure across 2013 IRF stays [11]. The new audit is expected to update the methodology and produce findings in 2026 or 2027.
Improper payment rates remain elevated. CMS's most recent data from the 2024 reporting period shows medical necessity errors accounting for 93.8% of improper payments at inpatient rehabilitation hospitals, with insufficient documentation accounting for the remaining 6.2% [3]. Rehabilitation units within acute care hospitals showed similar patterns — 86% medical necessity, 10.8% insufficient documentation [3]. These figures are the proximate driver of CMS's continued investment in IRF audit infrastructure.
For IRF CEOs and COOs, the practical takeaway: documentation that survives audit in 2026 needs to be structurally complete and consistently produced. Periodic compliance pushes don't survive structured review; continuous compliance does.
What's at Stake Financially
Sources: CMS FY2026 IRF PPS Final Rule [6]; CMS IRF QRP non-compliance policy [7]; payment per-discharge values from FY2026 final rule [6]. Annual exposure figures assume conservative 20% audit selection rates consistent with historical OIG sampling methodology [10].
The 2-percentage-point QRP reduction may sound modest, but it compounds across every Medicare discharge for a full fiscal year. For a typical 50-bed IRF processing 800 Medicare discharges annually, that's roughly $310,000 in lost reimbursement per year of non-compliance — recoverable only by demonstrating full compliance in the following reporting period [7].
For rehab hospital leaders ready to move from periodic compliance pushes to continuous, real-time schedule stability, Opmed's Rehabilitation solution is built specifically for IRFs — automating the daily compliance calculation across PT, OT, and SLP while reabsorbing refusals and cancellations as they happen. Book a demo and we'll show you exactly how the 900-minute calculation runs against your facility's specific staffing and patient mix.
How IRFs Move From 70–80% Compliance to 95%+
Across our customer base, IRFs that reach 95%+ reimbursement approval rates share four operational characteristics — and none of them are about adding scheduling staff [Opmed].
1. Real-Time Schedule Recalculation Instead of Nightly Rebuilds
Manual scheduling is fundamentally retrospective: yesterday's schedule rolls forward, gets adjusted overnight, and presents tomorrow's plan to a clinical team that's already three hours behind by 8:00 AM. Real-time recalculation flips the model — the schedule continuously rebalances as refusals, cancellations, and clinical changes happen. A patient refuses an 11:00 AM PT session; the system reslots OT into that window and rebuilds make-up minutes into the next 36 hours rather than waiting until the weekly compliance check fails.
2. 36-Hour Therapy Initiation as a Hardcoded Constraint
The 36-hour rule is a non-negotiable regulatory requirement, but in manual scheduling it's often a soft target — therapy starts when the team gets to it. When 36 hours becomes a hardcoded scheduling constraint that the system enforces against admission timestamps, late starts go from "common" to "exception." This single change typically improves Day-1 and Day-2 compliance rates by 15–25 percentage points within 30 days of implementation [Opmed].
3. Cross-Discipline Sequencing Built Into the Daily Plan
PT, OT, and SLP can't all happen at the same time, in the same room, with the same patient. Manual schedulers solve this conflict locally and break it globally. A model that treats the daily schedule as a constraint-satisfaction problem — sequencing across disciplines, staff, rooms, and patient tolerance simultaneously — produces 12% more billable hours per facility while improving treatment value by 13% [Opmed]. The pattern shows up at customer sites including Mayo Clinic, Geisinger, and Reuth Rehabilitation Hospital.
4. Therapist Schedule Predictability as a Retention Strategy
The reason burnout matters operationally is that it directly produces the schedule chaos that causes compliance failure. When therapists experience constant schedule changes, idle gaps, and last-minute reassignments, turnover follows — and turnover compounds the scheduling problem because new therapists need ramp time, mentoring, and patient handoffs that absorb additional schedule capacity. IRFs that stabilize daily scheduling typically see 29% improvements in provider utilization, which in turn reduces the schedule chaos that drives turnover in the first place [Opmed].
The operational logic is circular in a productive way: stable schedules retain therapists, retained therapists produce stable schedules, and stable schedules deliver compliant minutes across all 7 days of every rolling compliance window. Individual results vary by facility size, patient mix, and implementation scope.
Move from Reactive Compliance to Real-Time Schedule Stability
The 900-minute rule fails not because clinical teams can't deliver the care, but because intraday schedule drift, refusals, and make-up minute coordination compound faster than nightly manual scheduling can absorb [Opmed IRF Handout 2026]. CMS audit data tells us exactly where the failures cluster — medical necessity documentation drives 93.8% of improper payments in inpatient rehabilitation hospitals — and the operational answer is automation that reacts in real time, not nightly rebuilds [3]. For IRFs aiming to move from 70–80% compliance to 95%+ reimbursement approval, the difference comes down to having scheduling infrastructure that treats compliance as a continuously satisfied constraint rather than an end-of-week recovery exercise.
See how Opmed automates 900-minute compliance — book a demo →
Related Resources
Continue exploring IRF operations and AI-powered healthcare scheduling with these 5 resources from the Opmed team:
- Opmed Rehabilitation Solution — purpose-built scheduling automation for Inpatient Rehabilitation Facilities
- Solving the Puzzle of OR Scheduling Optimization with AI — the network-science foundation behind Opmed's optimization engine
- A Physician's Perspective on AI in Healthcare — Dr. Omer Trivizki on the operational role AI plays in healthcare delivery
- Opmed Time Savings Calculator — a 90-second estimate of recoverable hours for your facility
- Book a Demo — see Opmed running against IRF-specific workflows
Editorial Note
This article is for informational purposes for healthcare operations leaders and does not constitute clinical, legal, or financial advice. All compliance, reimbursement, and operational decisions should be made in consultation with qualified counsel, your facility's compliance team, and CMS guidance specific to your facility type and circumstances. CMS requirements and reimbursement structures are updated periodically; the figures and rules cited here reflect current guidance as of April 2026, and IRF leaders should always verify against the latest CMS publication at the time of operational decision-making. Opmed.ai is a healthcare operations platform; our outcomes data reflects aggregate performance across customer facilities and individual results will vary based on facility size, staffing, patient mix, and implementation scope.
Last reviewed: April 2026 by the Opmed Editorial Team.
References
[1] Medicare Benefit Policy Manual, Chapter 1, Section 110 — Inpatient Rehabilitation Facility (IRF) Services, Centers for Medicare & Medicaid Services, CMS Pub. 100-02, Rev. 10892 — https://www.cms.gov/files/document/r10892bp.pdf — accessed April 2026.
[2] Inpatient Rehabilitation Hospitals & Inpatient Rehabilitation Units — Provider Compliance Tips, Centers for Medicare & Medicaid Services / MLN, February 2026 — https://www.cms.gov/training-education/medicare-learning-networkr-mln/compliance/medicare-provider-compliance-tips/inpatient-rehabilitation-hospitals — accessed April 2026.
[3] 2024 IRF Improper Payment Reporting Period Data, Centers for Medicare & Medicaid Services, 2024 — https://www.cms.gov/training-education/medicare-learning-networkr-mln/compliance/medicare-provider-compliance-tips/inpatient-rehabilitation-hospitals — accessed April 2026.
[4] 42 CFR § 412.622(a)(3)(ii), Code of Federal Regulations — https://www.ecfr.gov/current/title-42/chapter-IV/subchapter-B/part-412/subpart-P — accessed April 2026.
[5] Review Choice Demonstration for Inpatient Rehabilitation Facility Services, Centers for Medicare & Medicaid Services, March 2026 — https://www.cms.gov/data-research/monitoring-programs/medicare-fee-service-compliance-programs/prior-authorization-pre-claim-review-initiatives/review-choice-demonstration-inpatient-rehabilitation-facility-services — accessed April 2026.
[6] FY 2026 Inpatient Rehabilitation Facilities Prospective Payment System Final Rule (CMS-1829-F), Centers for Medicare & Medicaid Services, August 2025 — https://www.cms.gov/newsroom/fact-sheets/fy-2026-inpatient-rehabilitation-facilities-prospective-payment-system-final-rule-cms-1829-f — accessed April 2026.
[7] Inpatient Rehabilitation Facility (IRF) Quality Reporting Program (QRP) Reconsideration and Exception & Extension, Centers for Medicare & Medicaid Services, March 2026 — https://www.cms.gov/medicare/quality/inpatient-rehabilitation-facility/irf-quality-reporting-reconsideration-and-exception-extension — accessed April 2026.
[8] Many Inpatient Rehabilitation Facility Stays Did Not Meet Medicare Coverage and Documentation Requirements (A-01-15-00500), HHS Office of Inspector General, October 2018 — https://oig.hhs.gov/reports/all/2018/many-inpatient-rehabilitation-facility-stays-did-not-meet-medicare-coverage-and-documentation-requirements/ — accessed April 2026.
[9] Inpatient Rehabilitation Facility Nationwide Audit (Work Plan), HHS Office of Inspector General, 2022–ongoing — https://oig.hhs.gov/reports/work-plan/browse-work-plan-projects/inpatient-rehabilitation-facility-nationwide-audit/ — accessed April 2026.
[10] Many Inpatient Rehabilitation Facility Stays Did Not Meet Medicare Requirements — Audit Report A-01-15-00500, HHS Office of Inspector General, October 2018 — https://oig.hhs.gov/oas/reports/region1/11500500.pdf — accessed April 2026.
[11] AHA Letter to HHS OIG Re: Inpatient Rehabilitation Facility Audit Report, American Hospital Association, December 19, 2018 — https://www.aha.org/system/files/2018-12/181219-aha-let-hhs-oig-audit-report.pdf — accessed April 2026.
[Opmed] Opmed.ai aggregate customer outcomes data, 2024–2026 — https://www.opmed.ai/
[Opmed IRF Handout 2026] Opmed.ai IRF Marketing Handout, 2026 — Opmed.ai

FAQs
What is the CMS 900-minute rule for IRFs?
The CMS 900-minute rule is industry shorthand for the intensive rehabilitation therapy requirement codified in the Medicare Benefit Policy Manual, Chapter 1, Section 110 [1]. It requires Inpatient Rehabilitation Facilities to demonstrate that patients are receiving intensive therapy at one of two thresholds: at least 3 hours of therapy per day across at least 5 days per week, or at least 15 hours of therapy (900 minutes) over a 7-consecutive-calendar-day period [1]. Therapy must include multiple disciplines — at least one of which must be PT or OT — and must begin within 36 hours of midnight on the day of admission [4].
Is the 900-minute rule the same as the 3-hour rule?
Yes. The "900-minute rule" and "3-hour rule" refer to the same regulatory requirement, expressed two different ways [1]. The 3-hour framing comes from the standard 3-hours-per-day-times-5-days path to compliance (15 hours per week). The 900-minute framing comes from the alternative 15-hours-per-7-day path, which equals 900 minutes. CMS allows both paths because some patients can't tolerate 3-hour daily therapy due to medical complexity but can still meet the weekly 15-hour threshold with a different distribution [1].
What happens if an IRF fails the 900-minute requirement?
When CMS, OIG, or a Medicare Administrative Contractor reviews an IRF claim and the documentation doesn't support that the patient received intensive therapy meeting the requirement, the entire stay's reimbursement can be denied or recovered through clawback [10]. The average FY2026 IRF PPS per-discharge payment is approximately $19,364, so each failed stay represents that level of risk [6]. Additionally, IRFs that fail the IRF Quality Reporting Program face a 2-percentage-point reduction in their Annual Increase Factor for the following fiscal year [7].
What is the IRF Review Choice Demonstration?
The Review Choice Demonstration is a CMS program requiring participating IRFs to choose between 100% pre-claim review or 100% postpayment review of Medicare claims [5]. CMS launched it in Alabama (August 2023) and Pennsylvania (June 2024), and announced expansion to Texas (effective March 2, 2026) and California (effective May 1, 2026) [5]. After six months of demonstrated compliance, IRFs become eligible for reduced-burden review options. The program affects roughly the largest concentration of IRFs in the United States.
How long do IRFs have to make up missed therapy minutes?
Make-up minutes must be delivered within the same 7-day rolling window in which they were missed in order to count toward intensive therapy compliance [1]. This is why intraday schedule drift compounds so quickly: a refusal on Tuesday morning that doesn't get reabsorbed by Sunday evening doesn't "carry forward" — it counts as a deficit for that 7-day window. CMS does provide a "Brief Exceptions Policy" allowing breaks of up to 3 consecutive days for documented clinical events (extensive diagnostic tests, surgical procedures, deep vein thrombosis bed rest), but the exception must be documented in the medical record [1].
Can AI scheduling tools help with 900-minute compliance?
Yes — and the operational mechanism is specific. AI-powered scheduling helps with 900-minute compliance by treating the daily schedule as a continuously rebalanced constraint-satisfaction problem rather than a nightly manual rebuild [Opmed]. When a refusal or cancellation occurs, the system immediately recalculates make-up minute placement across the rest of the 7-day window, factoring in therapist availability, patient tolerance, and cross-discipline sequencing. IRFs using this approach typically reach 95% reimbursement approval rates within 60–90 days of implementation, though individual results vary by facility size, patient mix, and implementation scope [Opmed].
What documentation does CMS require to support 900-minute compliance?
CMS requires the IRF medical record to include the preadmission screening, the post-admission physician evaluation, the individualized overall plan of care signed by a rehabilitation physician, weekly interdisciplinary team conference notes, evidence of at least 3 face-to-face rehabilitation physician visits per week, and therapy delivery documentation that supports either the 3-hour-per-day-5-days-per-week path or the 15-hour-per-7-day path [1]. The plan of care must specify the expected intensity (hours per day), frequency (days per week), and duration (total weeks) of interventions [1].
How is CMS changing IRF compliance requirements in FY2026?
The FY2026 IRF PPS Final Rule (CMS-1829-F) finalized a 2.6% increase to IRF PPS payment rates and made several changes to the IRF Quality Reporting Program [6]. CMS removed two COVID-19 vaccination measures, finalized the removal of four Social Determinants of Health standardized patient assessment data elements (effective FY2028), and amended the QRP reconsideration policy to permit extension requests for "extraordinary circumstances" [6]. The 900-minute therapy requirement itself was not modified in the FY2026 rule. CMS also expanded the Review Choice Demonstration to Texas and California, increasing the number of states under structured review [5].
%20(1).png)